Why TPA Claims Get Rejected — and How Hospitals Can Prevent It
-
A Comprehensive Practical Guide for Doctors, Hospitals, Billing Teams & Administrators in India
India’s health insurance ecosystem is rapidly expanding, but so are disputes between hospitals, TPAs, insurers, and patients.
Current operational realities show:
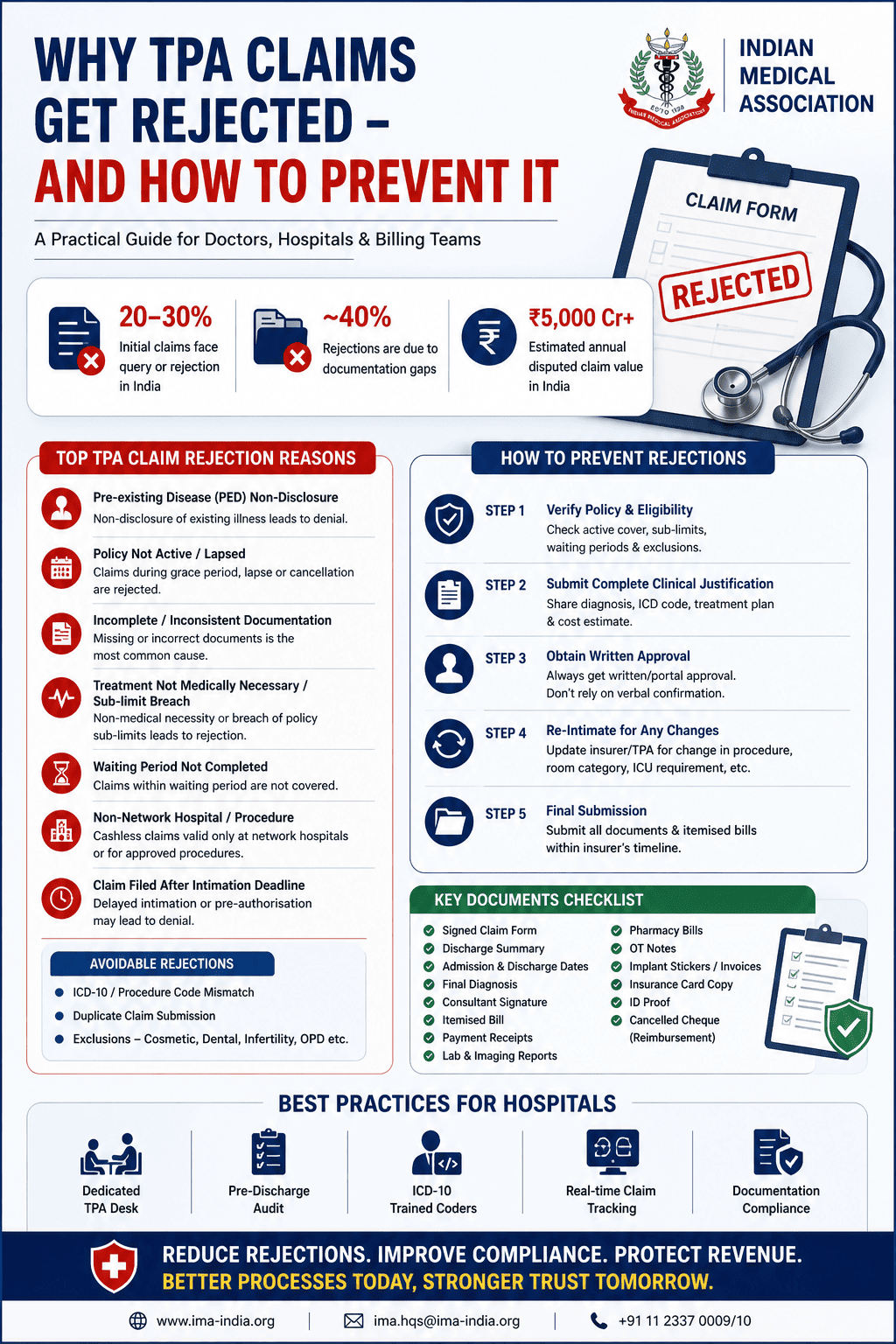
- Nearly 20–30% of initial insurance claims face queries, deductions, or outright rejection.
- Approximately 40% of claim disputes arise due to documentation gaps and operational errors, not because treatment was medically inappropriate.
- India’s annual disputed health insurance claim burden is estimated to exceed ₹5,000 crore.
Most claim losses are not caused by medical treatment itself — they originate from:
- Poor documentation
- Incorrect coding
- Delayed pre-authorisation
- Billing inconsistencies
- Operational miscommunication between departments
- Lack of structured TPA workflows
This guide combines:
- Regulatory and legal frameworks
- Practical hospital operations
- Real-world TPA rejection scenarios
- Department-level failures
- Preventive systems hospitals must implement
1. Understanding TPAs and Their Role
A Third Party Administrator (TPA) is an IRDAI-licensed intermediary that coordinates between:
- The patient (insured)
- The hospital
- The insurance company
Under the IRDAI (Third Party Administrators – Health Services) Regulations, 2016, TPAs are authorised to:
- Process claims
- Verify policy eligibility
- Arrange cashless hospitalisation
- Conduct document verification
- Audit hospital bills
- Coordinate network hospital empanelment
- Approve or deny claims based on policy terms
Understanding how TPAs evaluate claims is critical because even medically justified treatment can face rejection if operational compliance is weak.
2. Major Reasons Why TPA Claims Get Rejected
A. Pre-Existing Disease (PED) Non-Disclosure
What Happens
TPAs compare the current diagnosis with the original insurance proposal form.
If a patient had:
- Diabetes
- Hypertension
- Kidney disease
- Cardiac illness
- Spine problems
- Arthritis
before policy inception but failed to disclose it, the insurer may invoke:
- Material misrepresentation clauses
- Insurance Act provisions
- PED waiting period exclusions
Common Outcome
Claim rejected under:
- Non-disclosure
- Fraudulent declaration
- Pre-existing disease exclusion
Hospital Prevention Strategy
- Cross-check chronic illnesses during admission
- Compare patient history with policy declaration sheet
- Document physician notes clearly
- Avoid vague diagnosis descriptions
B. Policy Lapsed / Inactive During Admission
What Happens
Claims are rejected when:
- Policy renewal was missed
- Grace period is running
- Premium payment failed
- Policy expired before admission
Important Reality
Although IRDAI allows a 30-day grace period, treatment occurring during the grace period is generally not covered.
Prevention
-
Verify policy status before admission
-
Document:
- Date
- Time
- TPA verification reference number
-
Maintain screenshot/portal verification records
C. Incomplete or Inconsistent Documentation
The Single Largest Cause of Rejection
Common Missing Items
- Unsigned discharge summary
- Missing OT notes
- Illegible prescriptions
- Incomplete claim forms
- Missing consultant signatures
- Mismatch between admission & discharge diagnosis
- Missing investigation reports
Operational Reality
Many hospitals lose claims worth lakhs because:
- Junior staff complete files hurriedly
- Consultant signatures are pending
- Departments don’t coordinate
Prevention
Implement:
- Pre-discharge audit checklist
- Mandatory consultant sign-off
- Documentation verification before billing closure
D. Treatment Not Medically Necessary
Common Triggers
- Elective surgery shown as emergency
- Excessive investigations
- ICU admissions without justification
- Room rent beyond policy limit
- Unnecessary admission duration
What TPAs Do
Medical reviewers evaluate:
- Clinical necessity
- Standard treatment protocols
- Evidence-based indications
Prevention
Doctors must maintain:
- Objective clinical findings
- Proper admission indication
- Clear progress notes
- Justified ICU requirement
E. Waiting Period Not Completed
Standard Waiting Periods
Condition Type Typical Waiting Period General illness 30 days Cataract/Hernia 2 years Joint replacement 2–4 years Pre-existing disease 3–4 years Prevention
Before pre-authorisation:
- Verify policy inception date
- Check ICD-code related waiting periods
- Inform patient beforehand
F. Non-Network Hospital / Non-Empanelled Procedure
Common Scenario
Hospital is empanelled, but:
- Specific implant
- Robotic surgery
- Special procedure
- Advanced device
requires separate approval.
Prevention
Maintain:
- Updated TPA empanelment list
- Procedure-wise approval matrix
- Special approval workflow
G. Delayed Intimation
Standard Requirements
- Emergency admission: within 24–48 hours
- Elective admission: pre-authorisation mandatory
Ground Reality
Many hospitals delay intimation because:
- TPA desk unavailable
- Night admission confusion
- Weekend administrative gaps
Prevention
Create:
- Dedicated TPA desk
- 24/7 escalation workflow
- Emergency intimation SOP
3. Operational Realities That Cause Daily Rejections
Pharmacy Bills Not Matching Admission Dates
Real Scenario
Medicines purchased:
- Before admission
- After discharge
- During OPD visits
are merged into inpatient claim bills.
TPA Action
Entire pharmacy component may be rejected.
Prevention
Pharmacy software must:
- Tag UHID
- Link bills to admission episode
- Separate OPD & IP billing
Consumables Billed Improperly
Common Error
OT note:
- Gloves × 4
- Sutures × 2
But bill says:
- “Surgical kit — ₹12,000”
TPA Concern
No item-wise transparency.
Prevention
- Real-time OT consumable tracking
- Itemised billing mandatory
- Avoid lump-sum consumable packages
Room Category Mismatch
Most Dangerous Financial Error
Scenario
Policy covers:
- Single AC room
Patient admitted to:
- Deluxe room
- Suite
without documented upgrade consent.
TPA Consequence
Proportional deduction across entire bill:
- Doctor charges
- ICU
- Nursing
- Procedures
- Consumables
Prevention
Obtain:
- Written room upgrade consent
- Insurance implication acknowledgement
Outsourced Investigations Re-Billed Improperly
Common Practice
Hospital reissues outside MRI/lab bill under own letterhead.
TPA View
Potential fraud or concealment.
Prevention
Always:
- Attach original outside lab invoice
- Clearly mark outsourced services
- Avoid rebilling under hospital header
4. Orthopaedic & Surgical Claims — Where Most High-Value Queries Occur
Implant Sticker & Invoice Mismatch
Real Problem
- Trial implant sticker used accidentally
- Sticker lost
- Batch numbers don’t match supplier invoice
Result
TPA queries remain unresolved for weeks.
Prevention
Mandatory OT Protocol:
- Final implant sticker on case sheet
- Duplicate copy with billing
- Invoice attached before claim submission
Implant Cost Above NPPA / Insurer Cap
Common Scenario
Imported implants exceed:
- NPPA ceiling
- Insurer benchmark
No surgeon justification submitted.
Prevention
Surgeon should immediately document:
- Anatomical complexity
- Revision requirement
- Bone quality issue
- Why premium implant necessary
Procedure Code Mismatch
Example
OT note:
- Arthroscopy
Billing code:
- Knee replacement
Result
Automatic medical audit query.
Prevention
Coders must code ONLY from:
- OT notes
- Discharge summary
- Surgeon-confirmed procedure
Post-Operative Complication Readmission
Common Scenario
Readmission within 30–90 days:
- Infection
- DVT
- Hardware failure
Hospital files fresh claim.
TPA Interpretation
Related complication of earlier admission.
Prevention
- Declare honestly
- Link admissions properly
- Attach prior discharge summary
- Surgeon clarification note mandatory
5. Pre-Authorisation — The Most Critical Step
Step 1 — Verify Eligibility
Check:
- Active policy
- Sum insured
- Waiting period
- Sub-limits
- Exclusions
Step 2 — Submit Strong Clinical Justification
Include:
- ICD-10 diagnosis
- Proposed procedure
- Cost estimate
- Consultant registration details
Step 3 — Obtain Written Approval
Never rely on:
- Verbal approvals
- Phone confirmation
Step 4 — Re-Intimate Clinical Changes
If:
- Surgery changes
- ICU required
- Diagnosis evolves
update TPA immediately.
Step 5 — Final Submission
Submit:
- Itemised bill
- Discharge summary
- Reports
- Pharmacy bills
- OT notes
- Implant invoices
- Claim forms
within insurer timeline.
6. Standard Document Checklist for Every Claim
Mandatory Documents
- Signed claim form
- Discharge summary
- Admission/discharge dates
- Final diagnosis
- Consultant signature
- Itemised bill
- Payment receipts
- Lab & imaging reports
- Pharmacy bills
- Original prescriptions
- OT notes
- Anaesthesia notes
- Implant stickers/invoices
- FIR/MLC copy (if medico-legal)
- Insurance card copy
- Patient ID proof
- Cancelled cheque (reimbursement claims)
7. Why TPA Queries Never Get Resolved
Core Reason: Departmental Disconnect
Claims fail because:
- OT has sticker
- Billing has invoice
- MRD has case sheet
- Surgeon unavailable
- Nobody coordinates
The Result
- Query pending 30–90 days
- Claim closed
- Payment lost
- Patient angry
- Hospital revenue leakage
8. The Most Important Operational Lesson
TPA Claims Are Not Only Medical Processes
They Are Administrative, Legal, Documentation & Communication Processes.
A clinically successful surgery can still become:
- Financially disputed
- Legally challenged
- Operationally rejected
if documentation and workflow systems are weak.
9. Best Practices Hospitals Must Implement
Recommended Hospital Systems
Administrative
- Dedicated TPA desk
- Claim escalation SOP
- Daily pending query dashboard
Clinical
- Structured discharge summaries
- Standardised OT notes
- Implant tracking protocol
Billing
- ICD-10 trained coders
- Pre-discharge audit
- Item-level consumable billing
IT Systems
- UHID-linked pharmacy integration
- Automated document checklist
- Claim tracking dashboard
Legal & Compliance
- Room upgrade consent
- Procedure-specific informed consent
- Insurance limitation counselling
10. Claim Rejection Escalation Pathway
A rejection is NOT final.
Level 1 — TPA Representation
Submit written appeal within 15 days.
Level 2 — Insurance Grievance Cell
Mandatory insurer grievance redressal mechanism.
Level 3 — Insurance Ombudsman
Orders binding up to ₹30 lakh.
Level 4 — IRDAI IGMS / Bima Bharosa
Official regulatory grievance escalation.
References
Regulatory & Legal References
-
IRDAI (Third Party Administrators – Health Services) Regulations, 2016
Insurance Regulatory and Development Authority of India
Website: www.irdai.gov.in -
Insurance Act, 1938 (Amended 2015)
Ministry of Law and Justice, Government of India -
IRDAI Standardisation of Exclusions Guidelines, 2020
Circular Ref: IRDAI/HLT/REG/CIR/194/09/2020 -
IRDAI Protection of Policyholders’ Interests Regulations, 2017
Claim documentation norms -
General Insurance Council — Arogya Sanjeevani Policy Wordings, 2020
General Insurance Council of India -
ICD-10 Coding Guidelines for Empanelled Hospitals under PM-JAY
National Health Authority, Government of India, 2019 -
Insurance Ombudsman Rules, 2017 (Amended 2021)
Ministry of Finance, Government of India -
IRDAI Integrated Grievance Management System (IGMS)
https://igms.irda.gov.in -
Bima Bharosa Portal
https://bimabharosa.irdai.gov.in
Final Takeaway
The majority of TPA claim losses in India are preventable.
Most rejections are not because:
- the surgery was wrong,
- the treatment was unnecessary,
- or the hospital lacked competence.
They happen because:
- documentation breaks,
- communication fails,
- coding is inaccurate,
- departments work in silos,
- and operational discipline is weak.
Hospitals that build:
- strong documentation systems,
- trained TPA workflows,
- coordinated billing,
- structured coding,
- and proactive query management
will:
- reduce revenue leakage,
- improve cash flow,
- avoid patient disputes,
- and strengthen insurer relationships long-term.